I am delighted to say I have been invited to be an “Addiction Expert” with Addictionland and will be the expert blogger for the month of December 2014. So check me out there as well.
I am delighted to say I have been invited to be an “Addiction Expert” with Addictionland and will be the expert blogger for the month of December 2014. So check me out there as well.

The article I reposted yesterday Gambling with America’s health!
– mentioned how members of Gamblers’ Anonymous saw gambling addiction, or gambling disorder, as an emotional rather than financial disease. The addicted person “wants to escape into the dream world of gambling” and “finds he or she is emotionally comfortable only when ‘in action.’”
This very revealing statement “emotionally comfortable only when ‘in action’.’” ties in with what we have being proposing in this blog. That addicts of various varieties engage in motoric or repetitve behaviours prompted by a desire to alleviate emotional distress, that somehow motoric of repetitive, compulsive behaviours almost people these individuals “regulate” or control their emotions. In the language of treatment centres, they “fix their feelings” via these obsessive-compulsive activities.
So there must be an inherent emotional processing and regulation difficulty which prompts these addictive behaviours. As we have seen in previous blogs, the inability to regulate and process emotions appears to lead to a recruitment of more motoric or compulsive (sub-cortical) parts of the brain rather than goal-directed, action-outcome, prefrontal cortex part of the brain. This leads to less conscious decision making and more “automatic pilot” type of responding.
Is there evidence of this emotional regulation difficulty in gambling addicts as there appears to be with alcoholics and those with eating disorders? In fact, we will explore in future blogs how there appears to be an emotional regulation and processing difficulty at the heart of all these different addictive disorders.
In a study we have recently come across pathological gamblers reported significantly less use of reappraisal as an adaptive emotion-regulation strategy, and reported a greater lack of emotional clarity and more impulsivity than individuals in the healthy community comparison group. Pathological gamblers reported a greater lack of emotional awareness compared to the healthy control group and reported differences in access to effective emotion-regulation strategies compared to both comparison groups (1).
“Failures in control over gambling are likely to be influenced by individual coping styles. Problem-focused coping includes active and effortful problem solving, while emotion-focused coping includes escape and avoidance behaviours (Lazarus & Folkman, 1984). Scannell, Quirk, Smith, Maddern, and Dickerson (2000) suggested that loss of control over gambling is associated with emotion-focused coping such as avoidance or escape. This suggestion has been supported by evidence that gamblers demonstrate deficits in coping repertoires (McCormick, 1994) and some rely on gambling to provide an escape from personal or familial problems (Corless & Dickerson, 1989; Lesieur & Rosenthal, 1991). Finally, in a sample of adolescent gamblers, those identified as at-risk for developing pathological gambling behaviours were those who exhibited more emotion-focused coping styles (Gupta & Derevensky, 2001).
Gambling behaviours, therefore, seem to be associated with a deficit in self-control
processes that may be exacerbated by reliance on coping styles characterized by
avoidance and escape. At a more basic level, difficulties managing emotions effectively may contribute to the use of maladaptive coping strategies and result in failures in self regulation and impulse control. Optimal self-regulation relies on being able to focus on long-term goals in the presence of emotional distress that tends to shift attention to the immediate present (Tice & Bratslavsky, 2000). In addition, struggling with one’s feelings may deplete coping resources and leads to decreased self-control (Baumeister, Muraven, & Tice, 2000), leading to increased risk of disinhibited or impulsive behaviour.
Finally, individuals who are feeling acute emotional distress will likely wish to escape via activities that promise immediate pleasure (Tice, Bratslavsky, & Baumeister, 2001) and pathological gamblers often report using gambling to escape from negative mood states (Blaszczynski & McConaghy, 1989; Getty, Watson, & Frisch, 2000).
Emotion regulation refers to strategies to influence, experience, and modulate
emotions (Gross, 1999). Although there are several factors that influence whether a
certain emotion-regulation strategy is adaptive in a particular situation, certain strategies appear to be costly and maladaptive. For example, suppression or avoidance of emotions is associated with increased negative effect and anxiety, physiological activity, and physical pain (Campbell-Sills, Barlow, Brown, & Hoffman, 2006; Gross & Levenson, 1997; Levitt, Brown, Orsillo, & Barlow, 2004; Masedo & Esteve, 2007). Experimental investigations also support the notion that the effort of suppressing emotions drains mental resources (Richards & Gross, 2000), which could lead to decreased self-control.

Ricketts and Macaskill (2003) investigated several techniques that gamblers use to modify their emotions, one of which was the technique of ‘shutting off’ or using gambling in order to stop an unpleasant emotional state.
Patients who used the technique of ‘shutting off’ were often the ones who also reported poorly tolerating emotional discomfort (Ricketts & Macaskill, 2003).
According to Baumeister, Zell, and Tice (2007), emotional distress leads to an increase in self-awareness, which consequently leads to a desire to decrease ones self-awareness. but at the cost of self-regulation.
If one is unable to self-regulate, this could lead to an addiction or a relapse of an addictive behaviour (Sayette, 2004).
Measures of emotion regulation have proved helpful in identifying patterns of
emotional responding associated with a range of substance-dependent population.
Specifically, we investigated the association between emotion-regulation deficits and gambling pathology using two measures of emotion regulation, the DERS and the Emotional Regulation Questionnaire (ERQ; Gross & John, 2003). The ERQ examines the habitual use of two specific emotion-regulation strategies,
namely expressive suppression and cognitive reappraisal. The use of suppression reduces the outward expression of emotions in the short term, but is less effective in reducing emotions in the long term and is, therefore, considered a maladaptive emotion-regulation strategy (Gross, 1998; John & Gross, 2004). Cognitive reappraisal involves changing the meaning associated with a particular situation so that the emotional impact is altered (Gross, 1999; Siemer, Mauss, & Gross, 2007).
We hypothesized that pathological gambling would be associated with increased
habitual use of suppression and decreased use of reappraisal on the ERQ and deficits in emotion regulation across multiple domains on the DERS, the gambling group would rely more on suppression as a habitual emotion-regulation strategy and report increased difficulty regulating their emotions. We also predicted that the gambling group would report less use of reappraisal as an emotion-regulation strategy compared to the healthy control group.
As expected, we found a significant relationship between self-reported problem,
gambling behaviour, and negative effect as measured by the DASS, as well as deficits in emotion regulation as measured by the DERS
Contrary to expectations, we did not find a significant relationship between gambling behaviour – although the gambling group reported a greater lack
of awareness of their emotions so may account for the lack of association between self-reported gambling behaviour and suppression efforts. If gamblers demonstrate less awareness or insight into their emotional states, there may be less need to suppress emotions.
Gamblers have been shown to be prone to depression and anxiety (Beaudoin & Cox 1999; Black & Moyer, 1998; Vitaro, Arsenault, & Tremblay, 1999), substance dependence, and greater difficulty managing stress (Blaszczynski & Nower, 2002) and this may may further weaken inhibitory control and increase the already present propensity for pathological gamblers to make impulsive decisions (McCormick, Russo, Ramirez, & Taber, 1984).
Once a habitual pattern of gambling behaviours has been established, the combination of emotional vulnerabilities, conditioned responses, distorted cognitions, and decision-making deficits maintain the cycle of pathological
gambling. Blaszczynski and Nower (2002) suggest that such emotional vulnerabilities make treatment more difficult in this particular group of gamblers and emphasize the need to address these underlying vulnerabilities in addition to directly targeting gambling behaviours in therapy. It may, therefore, be of therapeutic benefit to specifically assess for and target emotion-regulation strategies in this population of gamblers.
Given the gamblers in the current study demonstrated limited access to effective strategies for managing difficult emotions, it may be important for clinicians to address coping strategies (including emotion-focussed strategies) as a part of any comprehensive treatment package.
It is also important that the clinician is aware of any deficits in emotion-regulation strategies to ensure that the client is prepared to guard against relapse, given that the ability to tolerate distress is associated with increased length of abstinence from gambling (Daughters et al., 2005).”
References
1. Williams, A. D., Grisham, J. R., Erskine, A., & Cassedy, E. (2012). Deficits in emotion regulation associated with pathological gambling. British Journal of Clinical Psychology, 51(2), 223-238.
Here I simply repost a very comprehensive review of the costs of gambling in the USA – “Gambling with America’s Health” –
this was written by
This article cites my friend and author Catherine Townsend-Lyon who discusses her personal experience of gambling addiction.
Publicly, Scott Stevens, a chief operating officer of a company in Steubenville, Ohio, was a well-regarded member of his community. A married father of three, he was active in his local Catholic church, involved with high school sports teams, and helped develop parks in the area. Privately, Stevens was addicted to gambling. First exposed to slot machines at a trade show in Las Vegas in 2007, Stevens became a regular slot player at the Mountaineer Casino, Racetrack, & Resort, about 30 minutes away in Chester, West Virginia. By 2010, he had embezzled $7 million from his employer to gamble, and when they found out, he lost his job. Stevens continued to gamble secretly for the next 10 months, going to Mountaineer nearly every day, drawing money from his family’s savings, his 401(k), and his children’s college fund.On August 13, 2012, that money ran out. In a suicide note to his wife, he wrote: “I know you don’t believe it, but I love you so much. I have hurt you so much. Our family only has a chance if I’m not around to bring us down any further.” That evening, Stevens asked his 13-year-old daughter to bring him his hunting bag from the attic. He drove to a local park he had helped develop and called 9-1-1. When the sheriffs arrived, he shot himself.
“This is one of the biggest public health issues in America today that no one has been paying attention to.”
“If it can happen to a guy as smart as he was, then it can happen to anybody,” said Indianapolis attorney Terry Noffsinger in a talk last November at Harvard Law School. Noffsinger, with other attorneys, is representing Stevens’ widow Stacy in a lawsuit filed last month against Mountaineer Casino, its parent company MTR Gaming Group, and slot machine maker International Game Technology, alleging they are liable for her husband’s suicide. The suit accuses both the casino and the slot designer of using predatory and deceptive tactics to profit from people with gambling problems, like Scott Stevens.
“Mountaineer Casino knew, or should have known, that the condition of disordered gambling, especially slot machine addiction, is associated with severe adverse health and other consequences for individuals and their families. Not only are gambling addicts like Scott Stevens liable to literally gamble away everything they own and end up in crippling debt, but also to become suicidal at far higher rates than the general population and even the population of persons addicted to substances such as illegal drugs and alcohol,” the suit states.

Although the suit’s success is not assured—the few other cases in this area have not succeeded—it is part of a growing movement of activists, academics, lawyers, and former gambling addicts who are trying to spotlight the health, economic, and social costs of legal gambling. This group believes the gambling industry preys upon vulnerable people, including low-income individuals, youth, and problem gamblers and that gambling availability is linked to larger societal problems like crime and economic inequality.
For its part, the gambling industry points to a record of funding research into gambling addiction and efforts to educate the public about problem gambling. They maintain that they offer a fun activity that most people can do without serious consequences.
The opening of new gambling venues shows no signs of slowing down, despite the planned closing of four casinos in Atlantic City and financial problems for casinos in other states. Last fall, New Yorkersapproved the building of up to seven casinos. Many other states are in various stages of building casinos. Some in the gambling industry are trying to legalize online gambling, which is currently allowed in only three states, Nevada, New Jersey, and Delaware.
A debate over the social and health costs of legal gambling has largely been sidelined even as availability has expanded dramatically in the last 25 years. This is not because of a lack of merit, say experts and activists, but because of the political power of the gambling industry. They allege that the industry has employed tactics in the same spirit as those of tobacco companies, which for many years misled consumers about the addictive properties of cigarettes and advertised to young people and other vulnerable consumers.
According to Les Bernal, the national director of Stop Predatory Gambling, a Washington DC-based nonprofit, “This is one of the biggest public health issues in America today that no one has been paying attention to.”
A few experts predict that as stories of gambling addiction become more common, suits like that of Stacy Stevens will increase and could even succeed, as tobacco lawsuits did. “Ultimately gambling will be linked to the increase in social costs, gambling will be linked to the problems it creates, just like smoking was ultimately linked to cancer,” says Dr. Earl Grinols, a professor of economics at Baylor University. “It can take a while.”
In the world of gambling, the most addictive property is electronic video gambling machines, often slots, which bring in 70 to 85 percent of the revenue for casinos. In some states, electronic video terminals are even available in other venues, like restaurants and bars. The machines do not typically have warning labels or cut offs for heavy users. Casinos aggressively market to frequent patrons, giving them complimentary flights, hotels, and other perks. Meanwhile, the success of state voluntary exclusion programs where problem gamblers sign up to ban themselves from casinos is unclear.

Today’s slots are not the old lever-operated “one-armed bandits” but video game-like terminals that keep users playing by deliberate design, according to Dr. Natasha Dow Schüll, an associate professor in the program of science, technology, and society at the Massachusetts Institute of Technology and the author of Addiction by Design: Machine Gambling in Las Vegas. “The particular addictiveness of modern slots has to do with the solitary, continuous, rapid wagering they enable. It is possible to complete a game every three to four seconds, with no delay between one game and the next. Some machine gamblers become so caught up in the rhythm of play that it dampens their awareness of space, time and monetary value,” writes Dr. Schüll in a New York Times commentary.
“A lot of people think it’s a tax on the stupid,” recovering gambling addict Kitty Martz told the Oregonian. “Really, we’re behaving exactly the way the machines want us to.”
The idea that gambling lends itself to addiction like drugs or alcohol has taken some time to be acknowledged. Until the 2013 publication of the fifth edition of the Diagnostic Statistics Manual, or DSM-5, problem gambling was classified as an “impulse control disorder” in the same category as pyromania and kleptomania, even though most clinicians who treated problem gamblers recognized it as an addiction, says Dr. Silvia Martins, an associate professor of epidemiology at the Columbia University Mailman School of Public Health.
These gamblers exhibit many of the same problems as other addicts. “Everything you see with substance abuse you can make an analogy to gambling problems,” Dr. Martins says, citing family strife, financial hardship, and struggles with depression or anxiety.
To gamble legally 40 years ago, one had to travel to Nevada, go to a racetrack, or live in one of the handful of states that offered lotteries. In most towns, the closest one came to a betting game was playing charitable Bingo at church. Video slot machines had not yet come to market.
For most Americans today, a casino is just a car ride away. There are about 1,400 of them in 39 states, and 43 states sponsor lotteries with games that are recognizable even to non-gamblers, like Mega Millions, Powerball, Pick 10, and instant scratch off tickets. In advertising to citizens, states use slogans like, “Hey you never know,” “Give your dreams a chance,” and “Believe in something bigger.” Hawaii and Utah are the only states that offer no forms of legal gambling.
Gambling addiction is often considered a small cost, one brought upon by the individual unwise gambler.
Casinos represent a substantial part of the nation’s economy and enjoy support from members of both political parties. In 2012, the industry took in $37 billion in gross revenue, employed 332,075 people, paid $13 billion in wages, and contributed $8.6 billion in taxes, according to the American Gaming Association. Many casinos are not just places to play blackjack and slots but to eat or take in live music and comedy acts.
In this environment, gambling addiction is often considered a small cost, one brought upon by the individual unwise gambler. “They think that it’s an easy painless way to raise revenue but they don’t see the other side of it,” says Arnie Wexler. Wexler quit gambling over 45 years ago after a nearly three-decade addiction and has since served as executive director of New Jersey’s Council on Compulsive Gambling. He also runs counseling services for compulsive gamblers with his wife, Sheila.

According to a conservative interpretation of the available research by the National Center for Problem Gambling, 1.1 percent or 3.4 million Americans have a pathological gambling disorder and 2 percent or 6.2 million engage in problem gambling, a less severe form of gambling addiction. (The term problem gambling is often used to refer to both problem and pathological gambling.) Internationally, prevalence is as low as .5 percent of the population in Denmark and the Netherlands and as high as 7.6 percent in Hong Kong, according to a 2012 review for the province of Ontario. Though problem gamblers are a minority of visitors to casinos, their spending accounts for anywhere from 35 to 50 percent of the revenues, according to several studies summed up in a paper by the Institute for American Values, a nonpartisan think tank that focuses on family and social issues.
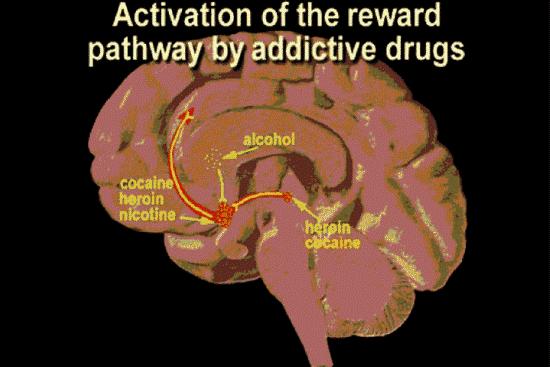
Neuroscientists have found commonalities between the brains of gambling and drug addicted people,like increased impulsivity and lower levels of activity in a region of the brain’s reward system, which leads people to seek bigger and potentially dangerous thrills. But it is not clear from this research when or how someone becomes addicted to gambling.
Compared to other nations, there has been relatively little epidemiologic research on rates of problem gambling in the U.S. The existing studies find that problem gambling increases with proximity to casinos. The federal government’s 1999 National Gambling Impact Study found that areas within 50 miles of a casino had twice as high a rate of problem gambling as those within 250 miles. The presence of a casino within 10 miles of a survey respondent’s home was positively related to problem or pathological gambling, according to a 2004 study by the University of Buffalo’s Research Institute on Addictions published in the Journal of Gambling Studies.
“If I were the gambling industry, I would want to fund people who had the disease point-of-view…because [they are] putting the source of problem gambling between the ears of the gambler.”

“Basically what we’ve learned is that as with many other kinds of environmental exposures, there typically is an increase in the prevalence rate of problem gambling in the wake of major introductions of new forms of gambling, whether it’s lotteries back in the 1980s and 1990s or casinos in the 1990s and 2000s,” says Dr. Rachel Volberg, a research associate professor of epidemiology at University of Massachusetts at Amherst and a researcher for the Massachusetts Gaming Commission. Dr. Volberg has found that rates of problem gambling began increasing during the most rapid expansion of gambling opportunities in North America and in Australia.
Yet she says problem gambling rates seem to level off after awhile. A study by the Research Institute on Addictions that has not been published yet found that rates of problem gambling did not continue to rise between 2010-2012 despite greater opportunity to gamble. Principal investigator Dr. John Welte, senior research scientist in psychology at the University of Buffalo, says it is not clear why, but he says it could be a result of the economic crisis.
The National Center for Responsible Gambling, or NCRG, is the charitable arm of the gambling industry’s trade association, called the American Gaming Association. NCRG cites a few studies that it says show problem gambling has not risen since the 1970s. After a casino moves in, problem gambling may become more widespread initially, but after a while, people “adapt”—they become more aware of the risks, seek treatment, or simply lose interest, says Christine Reilly, the senior research director of NCRG. This is called an “adaption effect.”
But prevalence studies do not tell the full story, says Dr. Stephen Q. Shafer, the chairman of the Coalition Against Gambling in New York. “One of the fallacies is that, let’s say you assume that your prevalence statistics are absolutely correct and you show that the prevalence of pathological gambling has not risen. It was, say, five years ago 1.1 percent. Last year it was 1.2 percent. What that forgets is that the prevalence is a pool out of which people move and into which people come, and looking at prevalence compared to time one and time two, you have to account for the people who have recovered, died, moved away.” For instance, a prevalence study conducted in 2008 would have counted Scott Stevens, but one in 2013 would not have.
For this reason, there need to be studies that use more rigorous epidemiologic methods, says Dr. Shafer, who is also a retired clinical professor of neurology and epidemiology at Columbia’s College of Physicians & Surgeons and the Mailman School. He has pushed to get New York State to commission such a study, but the state’s health department, the legislature, and the gambling commission have shown no interest.
Funding for gambling addiction research in the U.S. is about one-twentieth of funding in Australia and Canada, where gambling availability has also risen significantly in the past several decades, according to Dr. Volberg. Within the National Institutes of Health, there is an institute for research on alcohol disorders and an institute for research on drug addiction, but no institute for general addiction. Investigators who study problem gambling typically have to propose to look at it in conjunction with drug or alcohol use in order to win grants.
Gambling availability has other public health ramifications beyond addiction. It may exacerbate economic inequality, which has a strong relationship to health.
The NCRG is the only private funder of gambling addiction research in the country. According to Reilly, they fund research by top scientists at universities like Caltech, Duke, and Stanford, which are published in peer-reviewed journals. “We are funding some of the best people in the country, people who will lead us and force the issue at a national level,” says Reilly.
The majority of the NCRG’s funding goes to research based on a “disease model”—which investigates what goes on in the brains of individuals addicted to gambling—rather than the public health model, which looks at how availability affects population rates of problem gambling and potential social costs.
Both the disease model and the public health model “have points of truth, and they’re not mutually exclusive,” says Dr. Welte. But he adds, “If I were the gambling industry, I would want to fund people who had the disease point-of-view…because [they are] putting the source of problem gambling between the ears of the gambler.”
According to Reilly, the disease model is more practical because it can lead to treatments and that it is less prone to the flaws of survey research. “To me it seems kind of silly to spend time and money on an issue that is extremely difficult to research, because you can’t count on people’s memory,” she says.

But it is not in the gambling industry’s interest to have good research conducted on the social and economic costs of casinos and other forms of gambling, says Dr. Grinols. He points out that the federal government’s 1999 National Gambling Impact Study Commission recommended a moratorium on further gambling expansion until more research could be done on the economic and social costs and benefits. “No research of the type and focus hoped for by the Commission has been forthcoming since. That’s because the gambling industry has done what it could to question these studies and has not itself funded such studies,” says Dr. Grinols. “The whole conclusion of the Commission has been ignored and in fact thwarted by the failure of money to be available for good research.” Dr. John Warren Kindt, a business administration professor at University of Illinois whose research looks at the social and economic costs of gambling, calls what NCRG funds “pabulum research designed not to hurt the gambling industry and to misdirect the debate.” In response to such criticisms, Reilly is adamant that the NCRG has a totally independent review board, which she says mimics the structure of the National Institute of Health and does not interfere in the work of its researchers.
As for self-reporting, there are ways to validate responses. Dr. Robert Williams, a professor of addiction counseling at the University of Lethbridge in Alberta Canada, has compared what respondents report they spend on gambling to actual gambling revenue. He says the more reliable studies are those in which the total of the revenue reported by participants is closer to the total revenue made by the gaming industry. Dr. Williams points out that self-reporting may also underrepresent problem gamblers, who would be more likely to have their phone disconnected.
Gambling availability has other public health ramifications beyond addiction. It may exacerbate economic inequality, which has a strong relationship to health. It levies regressive taxes which take a larger share of income from lower than from upper income Americans. If taxes on gambling revenues substitute tax increases on income—which are progressive—the tax structure in a state becomes even more regressive. And those who spend money on certain forms of gambling are more likely to be low income.
There is “a strong positive relationship” between state lottery sales and the poverty rates, according toa 2007 study in the American Journal of Economics and Sociology by economists at Cornell University that looked at data over 10 years. The most typical lottery player is a black, male, high school dropout making less than $10,000 a year, according to a 1999 report to the National Gambling Impact Study commission. Problem gambling is significantly worse in economically disadvantaged areas according to two studies from 2013, one by Dr. Welte and his colleagues and another by Dr. Martins and her colleagues. And the presence of a casino is associated with rises in bankruptcy filings, according to a 2005 study from Creighton University.

While casinos may bring new jobs when they open, most are low-paying service work. The national median wage in the gambling industry is $10.76per hour. While better than some service jobs, it is less than the $16.87 hourly median wage for all industries, according to 2013 data from the Bureau of Labor Statistics.
And rather than boosting a local economy, casinos often draw business away from other food and entertainment venues. Many casinos are losing patrons to newer competition in neighboring states, straining state budgets and threatening local economies.
When casinos lose money or fail, the repercussions are significant. Delaware is spending hundreds of millions to keep struggling casinos afloat. In Atlantic City, several casinos plan to close by the end of the month, including the Revel, a two-year-old, $2.4 billion casino, entertainment, and conference center that was supposed to buoy the city’s flagging economy. The closures leave thousands of jobless peoplein a city that already has one of the highest unemployment rates in the country at over 15 percent as of April 2014, a violent crime rate six times the rest of New Jersey, and 29 percent of its population in poverty—a 7 percent increase since 1974, two years before New Jersey voters legalized gambling.
Although these statistics do not prove that the city’s gambling economy caused its problems, they do call into question claims by politicians and developers that casinos are an engine for economic growth. Nevertheless, some New Jersey politicians and business leaders are now talking about opening a new casino—or four—at the Meadowland Sport Complex in Bergen County, New Jersey.
Tribal lands that have casinos have seen improvement in jobs and county-level mortality rates,according to a 2002 study from the National Bureau of Economic Research. Yet these communities still see more bankruptcy, violent crime, and auto thefts and larceny after a casino opens.
Legal gambling is also linked to social problems like rises in crime and risky behavior in youth. Counties where casinos have opened have seen rises in the number of rapes, robberies, aggravated assaults, burglaries, larcenies, and auto thefts, compared with counties without casinos, according to a study by economists Dr. Grinols and Dr. David B. Mustard, which looked at county FBI data from 1977 to 1996.

Because children are now growing up in an environment where gambling is so widely advertised and available, they could be especially vulnerable. Youth are at greater risk for problem gambling than adults, according to a 2007 study from Canada. Two percent or about 750,000 teens ages 14 to 21 described gambling with three or more negative consequences in anational survey by Dr. Welte and colleagues in 2008. Another 11 percent gambled twice or more per week, which is considered frequent. Teen boys who gamble are more likely to become fathers before age 20, especially those who problem gamble, according to a study by Dr. Martins. African-American teens who are problem gamblers are more likely to have sex and get arrested at a younger age than those who don’t gamble. Teens who had depressive symptoms early in adolescence are more likely to have gambling problems later in adolescence, according to another Martins study from 2011.
Former U.S. Representative Robert Steele has observed the casino economy at work in southeastern Connecticut, the district he represented from 1970-75, which in the early nineties became home to both Foxwoods and Mohegan Sun Casinos.
The casinos created a “pervasive gambling culture.” He adds: “the people in southeastern Connecticut were in no way ready for the casinos.”
“They became almost instant successes and the two biggest casinos in the world,” says Steele, who has written a novel, The Curse, which is inspired by the story of the two casinos and the tribes behind them. With Atlantic City as their only competition in the Northeast United States, Foxwoods and Mohegan Sun drew about 60 percent of their customers from out of state and created 20,000 jobs.
But soon came problems no one seems to have anticipated. Drunk driving arrests in nearby Norwich more than doubled, and annual calls to the local police department went up fourfold, according to Steele. There was a sharp spike in the number of people who sought treatment for gambling addiction. The rate of embezzlement increased 400 percent, according to a report from the state. Steele’s own tax collector went to prison in 2001 for embezzling money from the town to gamble.
Much of the promised employment was in low-paying service jobs, sometimes part-time and often filled by non-English speaking workers who came from outside the area. This influx put pressure on local housing and social services. The local school system gained 400 children who collectively spoke 31 different primary languages, requiring them to create an “English for speakers of other languages” program. Teachers observed value changes in their students, says Steele. “[They] say, ‘we try to teach the kids the way to succeed in life is through hard work. Then the casino culture comes in and says, ‘you hit it big, you hit the lottery. You hit the payoff.’”
Today, revenue from Connecticut’s casinos is down 35 percent since its high point of 2007. Ultimately, says Steele, who used to have a property abutting Foxwoods, the casinos created a “pervasive gambling culture.” He adds: “the people in southeastern Connecticut were in no way ready for the casinos.”
“When everybody knows everybody, a good portion of the people you know are going to be affected—even if not directly—through broken homes, bankruptcy, the whole gamut,” says Dawley.

In Massachusetts, citizens are campaigning to repeal a deal that allows for MGM Resorts International to build an $800 million casino in the economically depressed town of Springfield. “We see this as very much a perpetuation of income inequality, and the implications that income inequality has on public health —that people stay in poverty basically, stay under-compensated. It’s the transfer of wealth from people who don’t have money to people who have abundant resources,” says Steven Abdow, a senior staff member of the Episcopal Diocese of Western Massachusetts. “This would be intentionally bring[ing] in a product that destroys lives.”
Abdow is working on a campaign to oppose the MGM casino. Once viewed as a way to revive the city’s dwindled fortunes, the casino’s fate is now in jeopardy. In June, a judge ruled in favor of ballot measure that would allow the citizens of Massachusetts to repeal a 2011 law that authorized casinos in the state.
Tyre, New York, is a town of less than 1,000 people 270 miles northwest of New York City. The town’s websiteboasts of a community that “strives to maintain its rural flavor,” welcoming visitors to stop by and visit the Montezuma National Wildlife Refuge and the Erie Canal. Last December, residents learned that a Rochester-based real estate company called Wilmorite was bidding to open the Lago Resort and Casino on agricultural land, across from an Amish farm.

“I grew up my whole life in this area. A casino certainly is not what you anticipate showing up on your doorstep,” says Jim Dawley, a resident whose property borders the proposed spot.
Dawley and his wife, who own and run a small manufacturing company, and two friends formed an organization called Casino Free Tyre to oppose Wilmorite’s plans. “When everybody knows everybody, a good portion of the people you know are going to be affected—even if not directly—through broken homes, bankruptcy, the whole gamut,” says Dawley.
Over 200 residents have signed a petition against the casino, but members of the town board are supportive of Wilmorite, which is promising multi-million dollar revenues. The Dawleys are not letting up, even though they are new to activism. “This is so far outside of my normal realm, it’s unbelievable. I have a little manufacturing business out in the woods. I’ve been involved in our church and things like that but as far as any political-rooted opposition, this is our first time.”
In the court case over the Massachusetts casino deal, an organization called the Public Health Advocacy Institute filed a friend-of-the-court brief that made a public health argument against the gambling industry. “Legalized casino gambling causes devastating effects on the public’s health, including not only the gambler but also their families, neighbors, communities and others with whom they interact,” the brief says. Electronic gambling machines “are designed to addict their customers in a way that is similar to how the tobacco industry formulates its cigarettes to be addictive by manipulating their nicotine levels and other ingredients.”
“Mirroring the tobacco industry’s strategy of creating scientific doubt where none truly exists, the casino industry has co-opted and corrupted scholarship on the effects of gambling through the use of front groups that funnel money to beholden scientists who are able to sanitize its origin,” the brief continues.
“The commercialization of a dangerous product that threatens both individual and public health has been called an ‘industrial epidemic,’” the brief continues, citing a 2007 paper published in the journalAddiction by Drs. René I. Jahiel and Thomas F. Babor. This is an epidemic “driven at least in part by corporations and their allies who promote a product that is also a disease agent.”
The brief argues that the citizens of Massachusetts have an interest in regulating gambling the way they have regulated cigarettes.
Given the power of the gambling industry and the dependence of states on gambling revenues, winning legal damages and regulating availability may presently seem like a pipe dream in the U.S. However, other countries employ harm reduction strategies in casinos to intervene on potential problem gambling,according to a 2011 report from the Cleveland Plain Dealer. In Holland, computers identify anyone who visits a casino more than 15 times a month as having a gambling problem. In the United Kingdom, casinos have to display the odds of winning on slot machines. And in Australia, there are limits on playing speeds and betting amounts.
The underlying principle behind this is articulated by Dr. Williams: “If provincial governments are going to make gambling available to their citizens, then concerted efforts are needed to prevent problem gambling, to effectively treat gambling addiction, and to minimize the amount of gambling revenue that comes from problem gamblers.”
People with gambling problems tend to elicit little sympathy. They are seen typically as exercising bad judgment when it is known that the “house always wins.” They have often hurt people they are closest to, both financially and emotionally.
“You don’t even have to be in action or sitting behind a machine because you’re constantly thinking about: When am I going to gamble? When am I going to win or lose? It just compounds.”
Former gambling addicts readily admit to their flaws. But, like most people, they typically started gambling because it was available, entertaining, and provided a potential if unlikely monetary reward. However, unlike most people who gamble, they became “hooked.” That’s how Catherine Townsend-Lyon speaks of her gambling addiction. She began playing video lottery terminals at delis and restaurants near her home in Grants Pass, Oregon, sometime after they were introduced in the 1990s. She became obsessed with a game called Flush Fever and soon began playing before and after work and during her lunch hour. She lied to her husband about her whereabouts and started secretly gambling their mortgage payments. She stole from the collection company she worked for and sometimes wore bladder control underwear so she wouldn’t have to get up to use the restroom while playing. When she lost money, she played to win it back, and when she won, she played to win more. In an extreme moment, she skipped the funeral of a close friend to drive 40 miles to an Indian casino so she could win enough money to prevent her home from being foreclosed. Instead, she lost everything. She drove home in tears and slit her wrists.

“It’s like a battle you have with yourself with the triggers and the urges and the obsessiveness. You don’t even have to be in action or sitting behind a machine because you’re constantly thinking about: When am I going to gamble? When am I going to win or lose? It just compounds. It’s exhausting. It’s never-ending,” says Townsend-Lyon, who, after seeking treatment several times, has managed to stay away from gambling for the last seven and-a-half years.
Townsend-Lyon says she turned to gambling at a difficult time in her life. With her husband frequently traveling for work, she found herself bored and looking for a way to fill the time. She had undiagnosed bipolar II disorder and had been sexually abused when she was younger but had not been raised to know to seek therapy. “I wasn’t a drug person or an alcoholic or anything like that, although I did drink more when I gambled. And because I was gambling, that was my coping skill. That’s what I was using to escape it, those feelings. I couldn’t stuff them away anymore. I would just use gambling to escape, not feel, zone out, you know what I mean?” she says.
She published a book last year about her former life, called Addicted to Dimes (Confessions of a Liar and a Cheat). What troubles her is how easy it is for people in her position to gamble. She didn’t have to fly to Nevada or even drive to a casino in state. The video poker and slot machines she played, which are sponsored by the Oregon State Lottery, are allowed at bars, restaurants, and delis.
“[I]f these machines weren’t in the bars and delis, then I would not be gambling. It’s that simple for me,” says a 33-year-old man quoted in a recent series on the state lottery by the Oregonian. He estimates he has lost $15,000 over 12 years from gambling. “That may sound like an excuse, but ‘out of sight is out of mind.’”

For people who are trying to recover from gambling addiction, it can be difficult to find help. Calls per month to the National Problem Gambling hotline are over two-and-a-half times what they were 14 years ago, from 9,642 in 2000 to 24,475 in 2013, according to Keith Whyte, executive director of the National Council on Problem Gambling. Yet funding for treatment centers, hotlines, and programs to prevent gambling addiction is minimal, says Dr. Martins. Funding for substance abuse treatment is about 281 times greater at $17 billion than public funding for problem gambling, at $60.6 million, although substance use disorders are only 3.6 times more common than gambling disorders, according to a 2013 survey by the Association of Problem Gambling Service Administrators and Problem Gambling Solutions. Just a little over half of the 50 U.S. states have someone whose full-time job is to administer problem gambling services, according to the same survey. By comparison, there are 113 lottery employees in Iowa and approximately 80 in Rhode Island. In several states legislators have cut gambling treatment funding or seen declines as a result of decreases in gambling revenue, which sometimes funds such programs, according to a Wall Street Journal report from 2011.
Gamblers’ Anonymous, a 12-step program modeled after Alcoholics’ Anonymous, is the most widely available and used treatment in the U.S. Members admit they are powerless over their gambling addiction and embark on changing their character through group meetings and the support of a “sponsor” or older mentor in the group. Little research exists on the efficacy of Gamblers’ Anonymous.A study from 1988 found that only 7.5 percent of members had abstained after one-year, and nearly a quarter of members did not go to a second meeting. However, those who regularly attend Gamblers’ Anonymous say they benefit significantly.
As with any kind of addiction, there is no pill for treating problem gambling. Medication and therapy may be used with varying success to treat a related psychiatric illness like depression or bipolar disorder. Moreover, a small number of problem gamblers seek treatment.
For these reasons, a public health approach, which would favor limiting the “exposure” of gambling to prevent addiction from occurring in the first place, is compelling. It is the same as the argument to tighten access to prescription opioids in order to prevent people from becoming hooked.
At a Gamblers’ Anonymous meeting in New York in August, about 65 people, mostly men, are celebrating one member’s five-year anniversary of abstaining from gambling. He gets to choose the topic for the night, and he picks “starting over.” Other members stand up to say that adhering to the Gamblers’ Anonymous program has fundamentally changed them. They have gone from being selfish and unable to make mature decisions to being better spouses, parents, friends, and members of society. They talk about small triumphs, their families, jobs, illness, and making amends with the people they hurt and stole from during their addiction.
“People adapt to their dislocation by finding the best substitutes for a sustaining social and spiritual life that they can, and addiction serves this function all too well.”
“I think it was known to pretty much everyone in this room that I was an asshole. And I think I have become a decent member of society,” says a man in his early 30s who has been abstinent for 10 years.
Another man echoes this sentiment. “I was anything but a good citizen,” he says. He has been abstinent for over 22 years, but like many others in this room, attends meetings on the Gamblers Anonymous principle that former addicts are always in recovery. “It’s not just starting over, we still have to own our past. We have to settle up with people as best we can.” When his mom passed away, he says he was grateful that he could access his emotions—not something he could have done in his gambling days.
“I can say without a doubt, gambling has ruined my life,” says another member. He has gone to Gamblers’ Anonymous for eight years but has had relapses, and it has been 201 days since he last bet. “Abstinence is for real this time.”
Compulsive gambling is often viewed as an addiction to money, but Gamblers’ Anonymous believes it is an emotional rather than financial disease. The addicted person “wants to escape into the dream world of gambling” and “finds he or she is emotionally comfortable only when ‘in action.’” But it doesn’t end up being much comfort, say formerly addicted gamblers who speak of how lonely their life was then.
Dr. Bruce K. Alexander, a psychologist and professor emeritus at Simon Fraser University in British Columbia, believes the loneliness experienced by those with gambling and other addictions has a strong social dimension. In his book, The Globalization of Addiction: A Study of the Poverty of the Spirit, he says: “A free-market society is magnificently productive, but it subjects people to irresistible pressures towards individualism and competition, tearing rich and poor alike from the close social and spiritual ties that normally constitute human life. People adapt to their dislocation by finding the best substitutes for a sustaining social and spiritual life that they can, and addiction serves this function all too well,” he says.

Bernal of Stop Predatory Gambling believes that our nation’s dependence on gambling reveals a deeper civic problem. “What we incentivize as a government shapes the national character,” he says. “We look at the greatest generation, we encouraged people to buy savings bonds, in the Great Depression. After World War II, we had the highest savings rate in modern American history because the government encouraged Americans to save. Today, half of Americans don’t own any assets.”
Terry Noffsinger, the lawyer for Stacy Stevens, admits that it has not been easy to make the legal public health case against gambling. Neither of the two cases he has represented has won in court, and one even provoked the Seventh Circuit Court of Appeals to threaten to sanction him for filing a frivolous claim. But he says the tide is turning. He has a conference call with a group of lawyers across the country about once a month to discuss the issue. Last November a group of Harvard Law students published a white paper making the case for legal action “to protect problem gamblers from the predatory behavior of casinos, including legislative reforms, tort litigation, regulations, and public policies.”
A couple of well-known trial attorneys have joined him on the Stevens suit, including Sharon Eubanks, who was lead counsel on the U.S. case that ended in a judgment in 2006 that the nation’s big tobacco companies fraudulently covered up the health risks of smoking and marketed to children. The Stevens case also makes product liability claims that the slot machines from which casinos draw so much revenue are intentionally designed, manufactured, and distributed to hurt people. Such claims have never been tried before.
“This is a blockbuster case. There are other cases that are starting to come out of the woodwork. The courts are ready to look more favorably upon addicted gamblers,” says Dr. Kindt of University of Illinois. Dr. Kindt published several academic articles in the early 2000s outlining the legal justification for mega-lawsuits against the gambling industry, similar to those which states, individuals, and classes of people filed against Big Tobacco.
In his Harvard talk, Noffsinger said he has had 100 or more people call him for help, many suicidal, nearly all of whom he has had to decline to represent. One of the calls came several years ago from a Boeing employee in Seattle who begged him for legal assistance. She had lost all of her money gambling, sold all of her furniture, and was ready to end it all. When Noffsinger told her he couldn’t represent her, she said she had nothing left to live for. Alarmed, he referred her to a lawyer friend in Seattle who found her counseling. About a year ago, she called Noffsinger and thanked him for saving her life.
“Somebody needs to do something…it may not be me.” Noffsinger told the Harvard students. “It’s going to be an uphill battle, but at the top there’s going to be a great big flag to wave.”
In treatment circles, I have constantly heard the refrain “one is not enough and two is too many!” and “the first drink gets you drunk” which points to a difficulty certain people have with stopping once they start drinking; a “loss of control” over drinking.
It is as if drinking gives you a thirst rather than taking it away. Many thousands of recovering alcoholics will tell you about this phenomenon – how they had only intended to have a couple but then lost a weekend to drinking instead.
It is an essential question to get to the bottom of, why do certain people not have the ability or have a reduced ability to stop once they start.
I came across an article from a few years back which addressed this issue (1) .
In those with a family history of alcoholism, drinking alcohol affects how the brain responds to an alcohol cue – in other words these individuals appear to want more compared to controls when they see alcohol cues. So drinking alcohol heightens a wanting for alcohol rather than causing a feeling of having had enough (not wanting).
Although a family history of alcoholism is the strongest risk factor for developing alcohol dependence, there are few studies of the association between familial alcoholism and the human brain’s reward system activity. This study used a functional magnetic resonance imaging (fMRI) to determine how family history affects the brain’s response to subjects’ preferred alcoholic drink odors (AO).
A family history of alcoholism doubles the odds of developing alcoholism (Hasin et al., 1997; Nurnberger et al., 2004). While environmental influences exert considerable influence in early adolescence, twin studies show an increasingly larger genetic influence by age 18 (Dick, Rose, & Kaprio, 2006), with a family history of alcoholism being a significant factor in the transition from abusive to dependent drinking (Hasin, Paykin, & Endicott, 2001).
While a number of studies have examined the human cerebral response to alcohol-related cues, particularly in alcoholics (e.g., Bragulat et al., 2008; Filbey et al., 2008b;Kareken et al., 2004; Myrick et al., 2008; Tapert et al., 2004;Wrase et al., 2007), very little research shows how familial alcoholism affects the brain response to alcohol-related cues— particularly in at-risk individuals who have yet to become dependent.

Animal research suggests that selective breeding for alcohol preference might affect the heavily dopaminergic mesocorticolimbic reward system. For example, rodents selectively bred to prefer alcohol have reduced dopamine in the striatum (see Murphy et al., 2002; Strother et al., 2005) and medial prefrontal cortex (Engleman et al., 2006), but greater striatal dopaminergic responses to alcohol itself (Bustamante et al., 2008; also see Smith & Weiss, 1999;Weiss et al., 1993). In at least one case, alcohol-preferring rats (compared to Wistar rats) showed a greater dopaminergic response in the ventral striatum during alcohol anticipation (Katner, Kerr, & Weiss, 1996). In non-abusive drinkers without a family history of alcoholism there is greater striatal dopamine receptor availability (Volkow et al., 2006), suggesting a potential protective factor.
Family history affects the brain’s response to alcohol’s olfactory (smell) cues in non-dependent, at-risk heavy drinkers and this study sought to determine how acute alcohol exposure affects the reward system’s response to alcohol’s conditioned cues by using intravenous (IV) alcohol infusion— a method that prescribes a constant level of brain alcohol throughout functional imaging and avoids the highly variable time courses of breath alcohol concentrations that accompany oral consumption (O’Connor et al., 1998; Plawecki et al., 2007;Ramachandi et al., 2004; Ramchandani et al., 1999).
So in effect alcohol was infused rather than simply drunk.
The researchers hypothesized that a family history of alcoholism would be associated with stronger responses to alcoholic drink aromas in the mesocorticolimbic reward system, and that a low-level of steady-state brain exposure to alcohol would potentiate these stimulus-induced responses (Bragulat et al., 2008). Such a potentiation could reflect a possible substrate for priming, when alcohol exposure increases desire to drink (De Wit, De Wit, 2000).
In this study (1) fourteen non-dependent heavy drinkers (HD) who were family history positive (FHP) participated, as did 12 HD who were family history negative (FHN). Subjects were imaged under both alcohol intoxication and placebo.
In this study alcohol intoxication dampened this “cued” response in the HD-FHP but potentiated (heightened) it in the HD-FHN.
This suggests that a family history of alcoholism and brain exposure to alcohol interact in heavy drinkers to differentially affect how the brain responds to alcohol cues.
In conclusion, frontal regions thought to process reward value may respond differently to alcohol’s classically conditioned cues in subjects with a family history of alcoholism. While alcohol appears to dampen medial frontal responses to alcohol cues in HD-FHP, it may enhance it in HD-FHN. Genetic background may therefore determine when, and under what circumstances, cues activate the reward network
References
Kareken, D. A., Bragulat, V., Dzemidzic, M., Cox, C., Talavage, T., Davidson, D., & O’Connor, S. J. (2010). Family history of alcoholism mediates the frontal response to alcoholic drink odors and alcohol in at-risk drinkers. Neuroimage,50(1), 267-276.
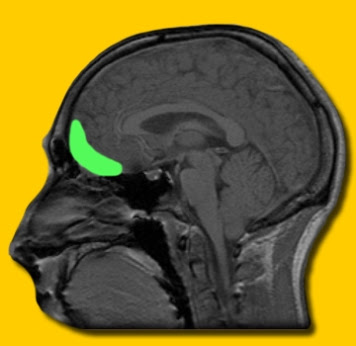
In the first of many blog on the commonalities in different additive behaviours we briefly consider whether there are brain mechanism similarities in different addictive of obsessive compulsive behaviours.

People affected by binge eating, substance abuse and obsessive compulsive disorder all share a common pattern of decision making and similarities in brain structure, according to new research from the University of Cambridge.
Researchers show that people who are affected by disorders of compulsivity have lower grey matter volumes (in other words, fewer nerve cells) in the brain regions involved in keeping track of goals and rewards.
In our daily lives, we make decisions based either on habit or aimed at achieving a specific goal. For example, when driving home from work, we tend to follow habitual choices – our ‘autopilot’ mode – as we know the route well; however, if we move to a nearby street, we will initially follow a ‘goal-directed’ choice to find our way home – unless we slip into autopilot and revert to driving back to our old home. However, we cannot always control the decision-making process and make repeat choices even when we know they are bad for us – in many cases this will be relatively benign, such as being tempted by a cake whilst slimming, but extreme cases it can lead to disorders of compulsivity.
In order to understand what happens when our decision-making processes malfunction, a team of researchers led by the Department of Psychiatry at the University of Cambridge compared almost 150 individuals with disorders including methamphetamine dependence, obesity with binge eating and obsessive compulsive disorder, comparing them with healthy volunteers of the same age and gender.
Study participants first took part in a computerised task to test their ability to make choices aimed a receiving a reward over and above making compulsive choices. In a second study, the researchers compared brain scans taken using magnetic resonance imaging (MRI) in healthy individuals and a subset of obese individuals with or withoutbinge eating disorder (a subtype of obesity in which the person binge eats large amounts of food rapidly).
The researchers demonstrated that all of the disorders were connected by a shift away from goal-directed behaviours towards automatic habitual choices. The MRI scans showed that obese subjects with binge eating disorder have lower grey matter volumes – a measure of the number of neurons – in the orbitofrontal cortex and striatum of the brain compared to those who do not binge eat; these brain regions are involved in keeping track of goals and rewards. Even in healthy volunteers, lower grey mattervolumes were associated with a shift towards more habitual choices.
Dr Valerie Voon, principal investigator of the study, says: “Seemingly diverse choices – drug taking, eating quickly despite weight gain, and compulsive cleaning or checking – have an underlying common thread: rather that a person making a choice based on what they think will happen, their choice is automatic or habitual.
“Compulsive disorders can have a profoundly disabling effect of individuals. Now that we know what is going wrong with their decision making, we can look at developing treatments, for example using psychotherapy focused on forward planning or interventions such as medication which target the shift towards habitual choices.”
References
http://medicalxpress.com/news/2014-05-creatures-habit-disorders-compulsivity-common.html#inlRlv
Voon, V et al. Disorders of compulsivity: a common bias towards learning habits. Molecular Psychiatry; E-pub 20 May 2014
Pornography triggers brain activity in people with compulsive sexual behaviour – known commonly as sex addiction – similar to that triggered by drugs in the brains of drug addicts, according to a University of Cambridge study published in the journal PLOS ONE.
Although precise estimates are unknown, previous studies have suggested that as many as one in 25 adults is affected by compulsive sexual behaviour, an obsession with sexual thoughts, feelings or behaviour which they are unable to control. This can have an impact on a person’s personal life and work, leading to significant distress and feelings of shame. Excessive use of pornography is one of the main features identified in many people with compulsive sexual behaviour. However, there is currently no formally accepted definition of diagnosing the condition.
Researchers from the Department of Psychiatry at the University of Cambridge looked at brain activity in nineteen male patients affected by compulsive sexual behaviour and compared them to the same number of healthy volunteers. The patients started watching pornography at earlier ages and in higher proportions relative to the healthy volunteers.
“The patients in our trial were all people who had substantial difficulties controlling their sexual behaviour and this was having significant consequences for them, affecting their lives and relationships,” explains Dr Valerie Voon, a Wellcome Trust Intermediate Clinical Fellow at the University of Cambridge. “In many ways, they show similarities in their behaviour to patients with drug addictions. We wanted to see if these similarities were reflected in brain activity, too.”
The study participants were shown a series of short videos featuring either sexually explicit content or sports whilst their brain activity was monitored using functional magnetic resonance imaging (fMRI), which uses a blood oxygen level dependent (BOLD) signal to measure brain activity.
The researchers found that three regions in particular were more active in the brains of the people with compulsive sexual behaviour compared with the healthy volunteers. Significantly, these regions – the ventral striatum, dorsal anterior cingulate and amygdala – were regions that are also particularly activated in drug addicts when shown drug stimuli. The ventral striatum is involved in processing reward and motivation, whilst the dorsal anterior cingulate is implicated in anticipating rewards and drug craving. The amygdala is involved in processing the significance of events and emotions.
The researchers also asked the participants to rate the level of sexual desire that they felt whilst watching the videos, and how much they liked the videos. Drug addicts are thought to be driven to seek their drug because they want – rather than enjoy – it. This abnormal process is known as incentive motivation, a compelling theory in addiction disorders.
As anticipated, patients with compulsive sexual behaviour showed higher levels of desire towards the sexually explicit videos, but did not necessarily rate them higher on liking scores. In the patients, desire was also correlated with higher interactions between regions within the network identified – with greater cross-talk between the dorsal cingulate, ventral striatum and amygdala – for explicit compared to sports videos.
Dr Voon and colleagues also found a correlation between brain activity and age – the younger the patient, the greater the level of activity in the ventral striatum in response to pornography. Importantly, this association was strongest in individuals with compulsive sexual behaviour. The frontal control regions of the brain – essentially, the ‘brakes’ on our compulsivity – continue to develop into the mid-twenties and this imbalance may account for greater impulsivity and risk taking behaviours in younger people. The age-related findings in individuals with compulsive sexual behaviours suggest that the ventral striatum may be important in developmental aspects of compulsive sexual behaviours in a similar fashion as it is in drug addictions.
“There are clear differences in brain activity between patients who have compulsive sexual behaviour and healthy volunteers. These differences mirror those of drug addicts,” adds Dr Voon.
Dr John Williams, Head of Neuroscience and Mental Health at the Wellcome Trust, says: “Compulsive behaviours, including watching porn to excess, over-eating and gambling, are increasingly common. This study takes us a step further to finding out why we carry on repeating behaviours that we know are potentially damaging to us. Whether we are tackling sex addiction, substance abuse or eating disorders, knowing how best, and when, to intervene in order to break the cycle is an important goal of this research.”
References
http://medicalxpress.com/news/2014-07-brain-sex-addiction-mirrors-drug.html
Voon, V et al. Neural correlates of sexual cue reactivity in individuals with and without compulsive sexual behaviours. PLOS ONE; 11 July 2014
Phillip Larkin – This Be The Verse
Looking back on my own childhood it is easier now to observe the fertile ground from which my genetic seeds of alcoholism started to flourish. I have long maintained that growing up in a dysfunctional family environment did not create my alcoholism but certainly did not help. A family environment were emotional expression was limited and veered between sentimentality and outright anger.
It is difficult to see how I learnt the essential adaptive skills of emotional regulation then; how to identify, label and express emotions freely without sanction, verbally, and non-verbally. For me emotions where something you cut off, experientially avoided, resisted. The more you did not let them get to you the tougher you were mentally somehow. Emotions were strangely dangerous things almost.
Emotions, having them, made you weak! People who indulged in them were weak.
I also grew up with a father who was a boxer and alcoholic (abstinent, thank God, via the local Church) who insisted emotions had to tolerated like a man, like some tough hombre in a 1950s Western. I had a host of uncles and a Grandad who agreed and they all set out to toughen me up. I even had boxing matches with cousins at various homes to show how I was progressing!
When I started drinking I found that this tough guy routine was greatly enhanced. Alcohol made me bullet proof. I drank and grew up to manhood in one go. Or so I thought – I didn’t realise that I stayed at that emotionally impaired 14 years old for nearly three decades later.
The worst effect on my emotional regulation skills was my relationship with my mother who struggled with valium abuse most of her adult life. This meant she was emotionally distant a lot of the time. Wose than that, she mixed mawkishness with being cold as a stone. It was an insecure attachment. You were never sure, emotionally, where you were at with her. It made me insecure, anxious and eventually very very angry. Cold blue angry.
But did this also have an effect on my ability to processing emotions. How could maternal emotional deprivation have an effect on my emotional processing skills? Andd how could this emotional processing difficulty affect the amount I craved alcohol??
I recently came across this article (1) which looked at this very question. I refer widely from it here.
Attachment theory is a widely used framework for understanding emotion regulation as well as alexithymia, and this perspective has also been applied to understand alcohol use disorders. One hypothesized function of attachment is the interpersonal regulation of affective experiences (Shaver & Mikulincer, 2007; Sroufe, 1977).
One hypothesized function of attachment is the interpersonal regulation of affective experiences (Shaver & Mikulincer, 2007; Sroufe, 1977). In the development of alexithymia, attachment theories stress the importance of significant others in childhood (Krystal & Krystal, 1988; Nemiah, 1977; Taylor et al., 1997). Evidence suggests that alexithymia is related to dysfunctional parenting (Thorberg, Young, Sullivan & Lyvers, in press).
Insecure attachment is associated with alexithymia and both harmful drinking and alcohol-dependence (Cooper, Shaver, & Collins, 1998; De Rick & Vanheule, 2006; Thorberg & Lyvers, 2006; Thorberg, Young, Sullivan, Lyvers, Connor & Feeney, 2009). In addition, alcohol abuse has been hypothesized to be a consequence of alexithymia (Taylor, Bagby, & Parker, 1997).
Research on alexithymia (1) has found significant positive associations between alexithymia, difficulties identifying feelings, difficulties describing feelings and alcohol problems (Thorberg, Young, Sullivan, & Lyvers, 2009; Thorberg, Young, Sullivan, Lyvers, Connor & Feeney, 2010). Individuals with alcohol-dependence and alexithymia report more severe alcohol problems compared to those with alcohol-dependence alone (Sakuraba, Kubo, Komoda, & Yamana, 2005; Uzun, Ates, Cansever, & Ozsahin, 2003). They also have poorer treatment outcomes (Loas, Fremaux, Otmani, Lecercle, & Delahousse, 1997; Ziolkowski, Gruss, & Rybakowski, 1995).
Individuals may use alcohol to escape feelings of rejection and establish a “secure attachment base” (Hofler & Kooyman, 1996), given alcohol’s stress and anxiety reducing effects.
![]()
In this study (1) results highlight the importance of alexithymia and difficulties identifying and describing feelings as related to preoccupation, obsessions and compulsive behaviors regarding drinking in those with alcohol-dependence. Or in more simple terms between alexithymia and craving. In this study 32.4% of this alcohol dependent groups were alexithymic. This is less than previously reported prevalence rates of 45-67% (Thorberg et al., 2009).
In this study (1) alcohol-dependence severity, alexithymia and insecure attachment were associated with more intrusive and interfering cognitions, ideas and impulses about alcohol, including an impaired ability to control these thoughts and impulses. This cognitively based “craving” as measured by the Obsessive Compulsive Drinking Scale (OCDS; Anton, Moak, & Latham, 1995), which is designed to assess obsessive thoughts and compulsive behavior toward drinking.
Hence there was a demonstrated relationships between alexithymia, craving, anxious attachment and alcohol problems in an alcohol-dependent sample. Higher levels of alexithymia led to a stronger desire for alcohol that was partially explained by an underlying mechanism, anxious attachment. One possible reason for this it may reflect an impairment in affect regulation.
Findings of the RAAS-Anxiety scale measured insecure attachment as related to a current or previous relationship, these findings may suggest that worries about being rejected, not cared for or unloved lead to an increased craving for alcohol.
One explanation for this mediational relationship may perhaps be that increased relationship stress is associated with a fear of intimacy and anxious attachment that leads to increased craving and perhaps a stronger attachment to alcohol. In other words, the alexithymia of insecure attachment may cause a stress dysregulation which prompts craving particularly as craving is a consequence of dysregulated stress systems. Stress dysregulations is also implicated in increased or more chronic alexithymia as suggested by George Koob in various articles. This has also been observed in other studies – this relationships of negative affect (anxiety, negative mood and emotion) with both alexithymia and craving (Sinha & Li, 2007).
To summarise, the results of this study support important relationships between alexithymia, difficulties identifying and describing feelings in relation to alcohol craving. These relationships extend to significantly higher levels of obsessive thoughts and compulsive behaviors in relation to alcohol use and alcoholism severity amongst individuals with combined alexithymia and alcohol-dependence, compared with alcohol-dependence alone. This study identified anxious attachment as a potentially important mechanism, in the relationship between alexithymia and alcohol craving.
References De Rick, A., Vanheule, S., & Verhaeghe, P. (2009). Alcohol addiction and the attachment system: an empirical study of attachment style, alexithymia, and psychiatric disorders in alcoholic inpatients. Substance use & misuse,44(1), 99-114.

Al-Anon Family Groups
In a word, “devastating.” That’s how Dr. George Koob describes the impact of a loved one’s alcoholism on family members and friends. Dr. Koob is the Director of the National Institute on Alcohol Abuse and Alcoholism (NIAAA), which is the leading funder of alcohol research in the world.
In this exclusive interview—released today—with Pamela Walters, Marketing Information Analyst for Al-Anon Family Group Headquarters, Inc., Dr. Koob is candid about concerns, not only for the person who drinks, but for those affected by the drinker.
“Children, particularly adolescents, but even younger children, friends and family members, all can be affected by an individual with an alcohol use disorder,” said Dr. Koob. He continued, “They often are experiencing negative emotions. They feel stressed. They feel alienated. They can become aggressive. These symptoms can lead to low self-esteem.”
In focusing on how children are affected by a parent’s drinking, Dr. Koob said, “About one in ten children in the United States lives with a parent with an alcohol misuse problem.” Dr. Koob commented on the subsequent, negative effects on a child’s development. Parents struggling with alcohol use disorders are sometimes “barely able to maintain themselves, much less take care of a child,” he said.
Dr. Koob continued, “We know that a child with a parent who binge drinks is much more likely to binge drink than a child whose parents do not binge drink. We know that it can lead to dynamics in the family that contribute to the development of alcohol use disorders in the children themselves, when they grow up.” He went on to reference research the Institute is conducting to get the word out about the family cycle of alcoholism, and to encourage those who are affected by a parent’s, or anyone’s, problem drinking to seek help from Al-Anon.
“I’ve had many of my colleagues over the years who joined Al-Anon because their parents had alcohol problems, and they found it very, very helpful for protecting them against their own vulnerabilities,” Dr. Koob said. He encourages friends and family members to get help for themselves in dealing with a problem drinker. “And that then can lead to a strengthening of yourself, but also of your ability to get help for intervention,” he said.
Find all of Dr. Koob’s comments in “NIAAA Director talks about the impacts of alcoholism on family members and friends,” as part of the “First Steps to Al-Anon Recovery” podcast series at al-anon.alateen.org.
The National Institute on Alcohol Abuse and Alcoholism is one of the 27 institutes and centers that comprise the National Institutes of Health (NIH). NIAAA supports and conducts research on the impact of alcohol use on human health and well-being. It is the leading funder of alcohol research in the world.
Al-Anon Family Groups are for families and friends who have been affected by a loved one’s drinking. Nearly 16,000 local groups meet throughout the U.S., Canada, Bermuda, and Puerto Rico every week. Al-Anon Family Groups meet in more than 130 countries, and Al-Anon literature is available in more than 40 languages. Al-Anon Family Groups have been offering strength and support to families and friends of problem drinkers since 1951. Al-Anon Family Group Headquarters, Inc. acts as the clearinghouse worldwide for inquiries from those who need help or want information about Al-Anon Family Groups and Alateen, its program for teenage members.
For more information about Al-Anon Family Groups, go to http://www.al-anon.alateen.org and read a copy of Al-Anon’s annual public outreach magazine “Al-Anon Faces Alcoholism 2015.”
Even as I a child I had difficulties controlling my impulses and my behaviours, “I was into everything”. I did not use much forethought in decisions making and would generally react and always be after something that I wanted desperately that very moment. Now in fact!
I believe I had sugar addiction, and chocolate and playing, and girl chasing addictive behaviours way before I ever got near alcohol in my early teens, with a six month, and quite disastrous period of poker machine gambling in between. And of course you couldn’t get me off the “Space Invader” machine. I just couldn’t get enough of anything, ever. Always wanted more, more and some more. My mother would call for me to come home in the darkening hours of evening. I had to be scraped off the playing fields in order to come home. Exhausted.
So why this constant overdoing of everything!!?
Why couldn’t I stop once in a while, ponder the consequences of my decisions, employ some, goal-directed, action-outcome type of thinking?
Following on for our very recent blog which described the neural mechanisms implicated in negative urgency we now look at at an article which attempts to bring together some of our most consuming research interests by attempting to explain whether there is a link between emotional processing deficits (alexithymia) negative urgency and dysregulated behaviours.
This study (1) looked at whether whether negative urgency (distress-based impulsivity) would be the link in relationship between alexithymia and dysregulated behaviors.
Dysregulated behaviors have been defined as behaviors that are difficult to control, and often result in functional impairment for the affected individual (Selby & Joiner, 2009).
An inability to understand affective and physiological experiences inherent in alexithymia might prompt individuals to engage in maladaptive behaviors in an effort to regulate emotions. One type of behavior linked to alexithymia is binge eating. Wheeler and colleagues (2005) found that alexithymia was positively correlated with binge eating in a sample of females.
Carano and colleagues (2006) found that alexithymia was positively correlated with the severity of binge eating behaviors. Additionally, Speranza and colleagues (2007) found that alexithymia predicted eating disorder treatment outcome in a three year prospective study meaning high levels of alexithymia can interfere with treatment response even more than the actual severity of the presenting problem.

Taylor and colleagues (1990) found that 50% of substance dependent males admitted to a drug and alcohol rehabilitation program were characterized as alexithymic. Similarly, Haviland and colleagues (1988) found that approximately 50% of individuals diagnosed as alcohol dependent were characterized as alexithymic. These numbers are significantly greater than the reported prevalence of alexithymia in the general population, which has been estimated to fall between 10 and 15% (Rybakowski et al., 1988; Parker et al., 1989), and suggests that alcohol and drug abuse is another example of a maladaptive behavior that may be used to modulate negative affective states when one is incapable of doing so in an adaptive way.
Loas and colleagues (1997) conducted a one year follow-up on individuals admitted to a psychiatric facility for alcohol treatment. Results suggested that individuals who remained abstinent from alcohol use one year post-treatment had
significantly lower scores on alexithymia measures.
“Why does the lack of understanding and expression of emotions have such a powerful influence over dysregulated behaviors?”
Why do individuals with high levels of alexithymia who experience negative affect seem to engage in dysregulated behaviors so frequently, while other individuals may simply cry, ruminate, or develop vegetative symptoms of depression?
Is negative urgency (Whiteside & Lynam, 2001; Cyders, Smith, Spillane, Fischer, Annus, & Peterson, 2007) the mechanism through which these behaviors are developed and sustained? It may be that the relationship between alexithymia and behavior is explained by a tendency on the part of individuals with high levels of alexithymia to act rashly in an attempt to immediately reduce psychological and physiological sensations associated with negative affect (negative mood, negative emotions, anxiety etc).
Negative urgency could be thought the mechanism that drives dysregulated behaviors in individuals who experience difficulty recognizing and expressing their emotions.

The authors (1) concluded that when faced with negative affect, many individuals are able to recognize and process their emotions adaptively. However, if people are not able to identify or describe their emotions (the very definition of alexithymia), our results suggest that this confusing affective experience may be quite upsetting (or unpleasant) and could lead to negative urgency, or a tendency to act rashly when they experience any type of negative affect.
High alexithymia individuals appear to be highly motivated to alleviate negative affect, regardless of the consequences. It may be that the emotional confusion inherent in alexithymia prompts individuals high on negative urgency to engage in dysregulated behaviors, by acting out either
against themselves or others.
—————————————————————————————————
As we mentioned in our previous blog emotional processing deficits are common in addiction and in other dysregualted behaviours and these deficits may not recruit the goal-directed parts of the brain. They do not guide action or choices effectively. As a result they manifest in perhaps crude, undifferentiated or processed forms as distress signals instead and recruit more limbic, motoric regions of the brain. Hence they are not used to anticipate future, long term consequence.
We disagree that it is not simply negative affect that prompts negative urgency but rather the chronic stress dsyregulation underpinning the manifestation of negative affect.
We are simply adding that as addiction becomes more chronic, so does stress and emotional distress and this appears to lead to a distress-based “fight or flight” responding to decision making. Addicts increasing appear to recruit sub-cortical or limbic areas in decision making and this is prevalent in abstinence as in active using. It is the consequence of chronic emotional and stress dysregulation.
References for this blog
Fink, E. L., Anestis, M. D., Selby, E. A., & Joiner, T. E. (2010). Negative urgency fully mediates the relationship between alexithymia and dysregulated behaviours. Personality and Mental Health, 4(4), 284-293.
In various blogs we have suggested that one of the main aspects of addictive behaviours is to act as the result of distress-based impulsivity or negative urgency. Here we explore in more details what we mean by that term negative urgency. Here we borrow from one article (1) which has an excellent review of negative urgency (1). The experience of emotion facilitates action. It has long been recognized that emotional processing appears to prepare the body for action (Frijda, 1986; Lang, 1993; Saami, Mumme, & Campos, 1998). In fact, to emote means, literally, to prepare for action (Maxwell & Davidson, 2007). Researchers have theorized that the relationship between emotional experiences and actions involve activation of the motor cortex by limbic structures (Morgenson, Jones, & Yim, 1980). Some investigations have used neuroimaging techniques to document increased activity in motor areas of the brain during emotional processing (Bremner et al., 1999; Rauch et al., 1996), and nonhuman studies suggest the emotion-action interface may involve connections between the amygdala and the anterior cingulate cortex (ACC: Devinsky, Morrel, & Vogt, 1995). Hajcak et al. (2007) found that emotionally arousing stimuli increase motor cortex excitability. The authors theorized that there may be individual difference in emotional reactivity that may relate to differences in the amount of activation of the motor cortex areas. One takes action to meet the need identified by the emotion.Pinker (1997) makes this point by noting that “Most artificial intelligence researchers believe that freely behaving robots . . . will have to be programmed with something like emotions merely for them to know at every moment what to do next” (p. 374). Intense emotions can undermine rational, advantageous decision making (Bechara, 2004, 2005;Dolan, 2007; Driesbach, 2006; Shiv et al., 2005). It also appears to be true that attempts to regulate negative emotions can impair one’s ability to continue self-control behaviors (Muraven & Baumeister, 2000; Tice & Bratslavsky, 2000; Tice,Bratslavsky, & Baumeister, 2001). Thus, it is not surprising that individuals engage in other strategies to manage intense emotions that are ill-considered and maladaptive, in that they work against one’s long-term interests. For example, heavy alcohol use may be used to manage emotion. Daily diary studies of alcohol use indicate that individuals drink more on days when they experience anxiety and stress (Swendson et al., 2000). Indeed, negative affect states have been shown to correlate with a greater frequency of many maladaptive, addictive behaviors, including alcohol and drug abuse (Colder & Chassin, 1997;Cooper, 1994; Cooper et al., 2000; Martin & Sher, 1994;Peveler & Fairburn, 1990). This pattern also is true of bulimic behaviors; individuals tend to participate in more binge eating and purging behaviors on days during which they experienced negative emotions (Agras & Telch, 1998; Smyth et al., 2007). Emotions such as shame, guilt, anger, depression, loneliness, stress, anxiety, boredom, and rejection are often cited as triggers for binge and purge episodes (Jeppson, Richards, Hardman, & Granley, 2003). For bulimic women, engaging in binge eating produces a decline in the earlier negative emotion (Smyth et al., 2007). Because actions like these do appear to reduce negative affect, they are reinforced. Brain Pathways Related to Emotion-Based Action Brain system involved in emotion and action -the amygdala, the orbitofrontal cortex (OFC) and its medial sector (the ventromedial prefrontal cortex, or VM PFC:Bechara, 2005), and other areas of the prefrontal cortex (PFC:Barbas, 2007). The amygdala appears to be heavily involved in the experience of negative affect; more broadly, it is thought to play a role in directing attention to emotionally salient stimuli, particularly stressful or disturbing stimuli (Davidson, 2003).
The OFC appears to be involved in the modulation of emotion-based reactivity (Davidson, 2003). OFC activity overrides emotional responses, apparently by providing information and a bias toward long-term, goal-directed behavior (Lewis & Todd, 2007). Davidson and his colleagues (Davidson, 1998, 2000,2003;Davidson & Irwin, 1999; Davidson, Putnam, & Larson, 2000) suggest the experience of intense emotion, and its accompanying potential actions, is inconsistent with one’s long-term goals. The OFC, perhaps particularly the left VM PFC, provides a biasing signal to avoid immediate reward, and thus maintain one’s pursuit of one’s longer-term goals. Davidson (2003) refers to this process as affect-guided planning and anticipation: with healthy left VMPFC functioning, one gains access to the emotion associated with anticipated outcomes consistent with one’s long-term goals. The ability to do so is, Davidson argues, the hallmark of adaptive, emotion-based decision making. At times, long-term affect-guided planning is difficult: the experience of intense emotions unrelated to one’s long-term interests may disrupt processing with regard to those interests (Gray, 1999; Preston, Buchanan, Stansfield, & Bechara, 2007). But healthy functioning of the left VM PFC helps one maintain an affective connection to one’s longer-term goals, and thus plan accordingly. Damage to the OFC, and perhaps damage specifically to the VM PFC, results in affective lability and rash action particularly in inhibiting the action of amygdaloid reactivity.
————————————————- The authors of this study put forward various reasons why OFC and VM PFC damage can cause rash action – we consider these before forwarding our own ideas of why OFC/ VM PFC damage may prompt distress based impulsivity. The OFC, perhaps particularly the left VM PFC, provides a biasing signal to avoid immediate reward, and thus maintain one’s pursuit of one’s longer-term goals. Davidson (2003) refers to this process as affect-guided planning and anticipation: with healthy left VM PFC functioning, one gains access to the emotion associated with anticipated outcomes consistent with one’s long-term goals. Activation of the left VM PFC also appears to inhibit amygdalar activity (Davidson, 1998), thus shortening the time course of the experience of negative affect and attention to stressful stimuli. Because negative affect stimulates autonomic nervous system (ANS) activity, which provides support for action in response to distress, prolonged negative affect leads to prolonged ANS arousal (Davidson, 2000). Perhaps a greater duration of ANS arousal increases the likelihood of affect-triggered action. Activity in the amygdala appears to facilitate this process. Damage to the OFC, and perhaps damage specifically to the VM PFC, results in affective lability and rash action. Individuals with PFC damage, and with OFC damage in particular, do not; they do not appear to have the normal anticipatory affective response to potential punishment (Bechara, 2004; Bechara, Tranel, Damasio, & Damasio, 1996; Cardinal et al., 2002). Thus, OFC damage appears to impair affective anticipation of potential risk to one’s actions. Bechara, Damasio, Damasio, and Anderson (1994) described OFC-damaged individuals as oblivious to the future consequences of their actions, but sensitive to immediate reinforcement and punishment. Thus, their actions tend to be guided by immediate consequences only. These patients had otherwise retained their intellectual capacities, including abstract reasoning skills. They could even describe possible future consequences in realistic language. They appeared simply to lack the anticipatory affect that others have; thus perhaps lacking the affect-guided anticipation described byDavidson (2003). The authors then suggest that associations between the OFC/VM PFC-amygdala system and psychopathy are consistent with their claim of an association between this system and the urgency traits. In other words, individuals high in psychopathy have reduced VM PFC functioning, and hence lack an affective connection to the consequences of their actions. Other studies have also documented similar OFC functioning deficits among psychopaths (Blair et al., 2006; Mitchell, Colledge, Leonard, & Blair, 2002). This model is interesting but there is not mention of stress systems in this model although the authors mention distress and negative affect but not the stress chemicals underpinning these affective manifestations. The authors also do no mention two hugely important points we believe; a. that this amgydaloid (hyper) activity, caused by PFC dysfunction can also “offline” PFC activity (fig.1) b. in favour of the compulsive, emotive-motoric behaviour of the dorsal striatum which drives rash action, distress-based impulsivity or compulsivity rendering the individual remote to negative consequence of actions, although he/she may be able to explain clearly these consequences. prior to or after seeming to not consider them. It is chronic stress dysregulation in addiction that “cuts off” access to action-outcome or goal-directed parts of the brain and recruits stimulus response, implicit, “must do” action instead. fig 1.
This we believe is the mechanism of negative urgency rather than as the authors suggest in this article, but not included, that VMPFC damage renders individuals unknowing of consequence, when rather, consequence, negative or otherwise, has been cut off by this amygdaolid activity rendering action outcome associations remote to consciousness. The brain acts implicitly, procedurally or in a stimulus response way to distress we believe in addictive disorders when heightened amgydaloid reactivity is in charge of behaviour with VMPFC deficit contributing to this amgydaloid dysfunction. An argument against simply seeing rash behaviour as the result of OFC or VMPFC damage which leads to lack of knowledge of consequence is that it does not really consider the chronic stress that accompanies addictive behaviours and which creates a near constant distress which acts in the way we describe above. This does not mean that there is a lack of emotionally guided behaviour or action on the part of addicts. It would appear, as discussed in previous blogs, that emotional processing deficits are common in addiction and may not recruit the goal-directed parts of the brain as the authors suggest. They do not guided action or choices effectively. As a result they manifest in perhaps crude, undifferentiated or processed forms as distress signals instead and recruit more limbic, motoric regions of the brain. Hence they are not use to anticipate future, long term consequence. We are simply adding that as addiction becomes more chronic, so does stress and emotional distress and this appears to lead to a distress-based “fight or flight” responding to decision making that the authors have mentioned in this article but not elucidated as above. Addicts increasing appear to recruit sub-cortical or limbic areas in decision making and this is prevalent in abstinence as in active using. it is the consequence of chronic and stress dysregulation. We suggest that this chronic stress prompts negative urgency via an hypofunctioning ACC (2) and by a “emotional arousal habit bias” as seen in post traumatic stress disorder (3) whereby chronic emotional distress increasingly during the addiction cycle comes to implicitly activate dorsal striatal responding “offlining” the PFC in a similar manner to fig. 1. References 1. Cyders, M. A., & Smith, G. T. (2008). Emotion-based dispositions to rash action: positive and negative urgency. Psychological bulletin, 134(6), 807. 2. Li, C. S. R., & Sinha, R. (2008). Inhibitory control and emotional stress regulation: neuroimaging evidence for frontal–limbic dysfunction in psycho-stimulant addiction. Neuroscience & Biobehavioral Reviews,32(3), 581-597. 3. Goodman, J., Leong, K. C., & Packard, M. G. (2012). Emotional modulation of multiple memory systems: implications for the neurobiology of post-traumatic stress disorder.
|